It is not just maternity care. It is the entire health care industry. Did you see this movie on CNN? It is now, in part, on You Tube and on iTunes. Here is a trailer and a link to the You Tube site.
What are your thoughts?
http://www.youtube.com/user/EscapeFireMovie/videos?flow=grid&view=1
Tuesday, March 26, 2013
Tuesday, March 19, 2013
Dare to Be Extreme
Reuters Newswire posted an article on 3/13/13 regarding hospital designation as Baby Friendly and the impact of that designation on initial and long-term breastfeeding rates.
"The paper shows that components of the BFHI steps are important for breastfeeding continuation and are more important than whether a hospital has BFHI accreditation or not," wrote Wendy Brodribb, the study's lead author from The University of Queensland, in an email to Reuters Health.
The bottom line is that saying you are baby friendly or that you have mother friendly staffers or that you believe in moms and babes isn't enough. Everyone has to agree that physiologic care of laboring/new mothers and newborns is the best practice.
So they don't all agree? No it is not that simple. It is complicated and convoluted. As I have mentioned countless times before, it is all about education. That is the key. Nurses and physicians are not taught physiologic care in schools. Hospitals don't have time to either teach physiologic care in in-service education or don't want to because, let's face it, physiologic care takes time. Time which hospitals don't have to spare. And expectant parents don't know about physiologic care so.............................you see the complexity of the problem?
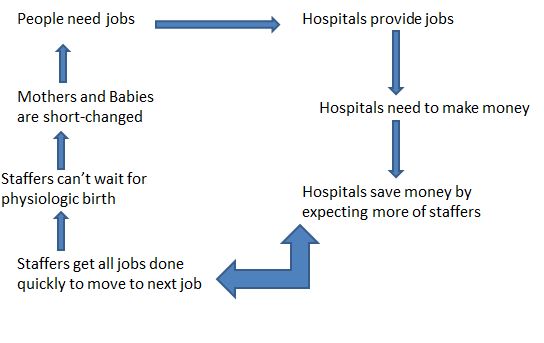
 The above graphic attempts to simplify the problem in a very one dimensional way. It would take a huge effort on the part of many to bring about the change necessary in maternity care. Think about the organization(s) through which you hold membership(s). Do they advocate for evidence-based physiologic care? If so how and to what degree? Preaching to the choir is necessary to maintain good energy to all of the troops. But also, take that energetic message to others. Sharing that message with other like-minded organizations is necessary. Urge your organization(s) to reach out and join with other organizations to stand together.
The above graphic attempts to simplify the problem in a very one dimensional way. It would take a huge effort on the part of many to bring about the change necessary in maternity care. Think about the organization(s) through which you hold membership(s). Do they advocate for evidence-based physiologic care? If so how and to what degree? Preaching to the choir is necessary to maintain good energy to all of the troops. But also, take that energetic message to others. Sharing that message with other like-minded organizations is necessary. Urge your organization(s) to reach out and join with other organizations to stand together.
Don't be tempted by apathy and complacency.
Dare to be extreme.
We must not overlook the role that extremists play. They are the gadflies that keep society from being too complacent.
"The paper shows that components of the BFHI steps are important for breastfeeding continuation and are more important than whether a hospital has BFHI accreditation or not," wrote Wendy Brodribb, the study's lead author from The University of Queensland, in an email to Reuters Health.
The bottom line is that saying you are baby friendly or that you have mother friendly staffers or that you believe in moms and babes isn't enough. Everyone has to agree that physiologic care of laboring/new mothers and newborns is the best practice.
So they don't all agree? No it is not that simple. It is complicated and convoluted. As I have mentioned countless times before, it is all about education. That is the key. Nurses and physicians are not taught physiologic care in schools. Hospitals don't have time to either teach physiologic care in in-service education or don't want to because, let's face it, physiologic care takes time. Time which hospitals don't have to spare. And expectant parents don't know about physiologic care so.............................you see the complexity of the problem?
Don't be tempted by apathy and complacency.
Dare to be extreme.
We must not overlook the role that extremists play. They are the gadflies that keep society from being too complacent.
~Abraham Flexner
Friday, March 15, 2013
How do we go about changing the culture of birth?
I am inspired by this quote:
Never doubt that a small group of thoughtful, committed, citizens can change the world. Indeed, it is the only thing that ever has.”
 Childbirth education - begin with women. Then move to student and existing OBs and nurses for education about physiologic birth. Once the information is out and embraced, as in the 70s, hospitals will have to comply with the wishes of the women...the consumers. Midwives will take their rightful place as providers of care for low risk women and OBs (the surgeons) will rightfully care for the high risk mothers. Hospitals will actually save money, US maternal/infant morbidity and mortality statistics will improve.
Childbirth education - begin with women. Then move to student and existing OBs and nurses for education about physiologic birth. Once the information is out and embraced, as in the 70s, hospitals will have to comply with the wishes of the women...the consumers. Midwives will take their rightful place as providers of care for low risk women and OBs (the surgeons) will rightfully care for the high risk mothers. Hospitals will actually save money, US maternal/infant morbidity and mortality statistics will improve.
Never doubt that a small group of thoughtful, committed, citizens can change the world. Indeed, it is the only thing that ever has.”
I attended a film showing of the classroom edition of the "Business of Being Born" at the University of Cincinnati last night. I had seen the movie before. Many times. I've met many of the people in the movie ~ Robbie Davis-Floyd, Ricki Lake. But I looked at it through new eyes. The eyes of the college women in attendance.
Their questions hit me to my core. "I want to talk to my gyn about my body BEFORE I start even thinking of pregnancy." "Why is there such a disconnect" (when speaking about the US's pitiful maternity statistics). And from one of the veteran women in the crowd - "I thought when I gave birth in the 70s that my daughters would have it better than me. What happened?"
What happened indeed. That seemed to be the question of the night! How do we go about changing the culture of birth?
Here is how I see the culture of birth in this country:
Birth is still a vital life experience to all women, regardless. They are not taught about their bodies, pregnant or non-pregnant.
Obstetricians are caring and skilled individuals. They are not taught about "normal" or physiologic birth.
Nurses are also caring and skilled individuals. They are not taught about "normal" or physiologic birth.
Midwives are caring and skilled individuals and ARE taught about "normal" or physiologic birth. In many states, midwives are underutilized and in the case of non-nurse midwives, outlawed.
Childbirth educators who could teach the women are minimalized by the OBs and nurses, whom they could also learn from via in-service education led by the childbirth educators.
OBs and nurses (and some midwives) work for hospitals which are businesses and in the words of Suzanne Arms, hospitals are designed for the mass care of the masses. Not the individual care of the individual.
Childbirth education programs are always on the chopping block, even in times of economic prosperity but always during tough economic times.
So we basically have a situation where careproviders who are not taught about "normal" or physiologic birth are working for an institution who needs, by definition, to make money and care for women who are not taught about "normal" or physiologic birth but often do want that type of birth.
How I see changing the culture of birth:
Childbirth education - begin with women. Then move to student and existing OBs and nurses for education about physiologic birth. Once the information is out and embraced, as in the 70s, hospitals will have to comply with the wishes of the women...the consumers. Midwives will take their rightful place as providers of care for low risk women and OBs (the surgeons) will rightfully care for the high risk mothers. Hospitals will actually save money, US maternal/infant morbidity and mortality statistics will improve.
Now, that wasn't so hard. Was it?
Thursday, March 07, 2013
Analysis of the Wide Variation In Cesarean Birth Rates in US Hospitals: Another Call for Childbirth Education
Implied. Under the
radar. Hinted at. All of these can be used to describe the
latest in a flurry of articles suggesting that childbirth education be ramped
up and that evidence-based information be more readily available to pregnant
women.
For example:
In the United States, childbirth is the most common reason
for hospitalization…and it often brings in a substantial portion of revenue for
the hospital. With the current US
cesarean rate wavering at 32.8%, it is any wonder that an examination of the
drastic variation in rates among hospitals has been launched.

In a recent article published in HealthAffairs, authors Katy Backes Kozhimannil, Michael Law and
Beth Virnig worked with data from 2009 and examined 593 US hospitals. They found that cesarean birth rates varied
tenfold across hospitals – from 7.1% to 69.9%.
Among this group of women with lower-risk pregnancies, in which more limited variation might be expected, hospital cesarean rates varied fifteenfold, from 2.4 percent to 36.5 percent.
"We were surprised to find greater variation in hospital cesarean rates among lower-risk women. The variations we uncovered were striking in their magnitude, and were not explained by hospital size, geographic location, or teaching status," said lead author Katy B. Kozhimannil, Ph.D., assistant professor in the University of Minnesota School of Public Health. "The scale of this variation signals potential quality issues that should be quite alarming to women, clinicians, hospitals and policymakers."
Kozhimannil and her colleagues suggested recommended four
major policies to reduce variations:
More and better data on the quality of maternity care are needed to support the rapidly advancing clinical evidence base in obstetrics. Clinicians and hospitals cannot improve maternity care, and insurers cannot pay for such improvements, without clear and consistent measures of quality.
Tying Medicaid payment policies to quality improvement programs may influence hospital policies and practices and provide incentives and reward hospitals and clinicians for providing consistent, evidence-based care.
Finally, information about cesarean rates and maternity care should be more readily available to pregnant women, who have time, motivation, and interest to research their options. However, they lack access to unbiased, publicly-reported information about cesarean delivery rates and other aspects of maternity care.
Yet, another clear mandate for the need for childbirth education.
And not childbirth education in the form of
regurgitated hospital expectations and current policy…”unbiased,
publicly-reported information about cesarean delivery rates and other aspects
of maternity care.”
Kozhimannil et al. Cesarean Delivery Rates Vary Tenfold
Among US Hospitals; Reducing Variation May Address Quality and Cost
Issues. Health Affairs March 2013, Vol. 32, No. 3.
Tuesday, March 05, 2013
A Favor and a Survey

Please use the link below & thanks in advance!
Click here to take survey
Subscribe to:
Posts (Atom)